Most dental problems announce themselves. A toothache, a cracked filling, an abscess; these things produce pain that eventually becomes impossible to ignore. Gum disease doesn’t follow that pattern. In its early stages, the stages where treatment is most straightforward and outcomes are most complete, it produces signs that are genuinely easy to dismiss.
Bleeding when brushing gets attributed to technique. Puffiness along the gum line is assumed to be temporary. Bad breath gets managed with mouthwash rather than investigated. None of these explanations are unreasonable. They’re just frequently wrong.
The difficulty with gum disease isn’t that the signs are invisible. It’s that they’re easy to rationalize away before they’ve been properly assessed. By the time the condition causes discomfort or visible damage, it has usually been developing quietly for considerably longer.
Why Most People Don’t Notice It Until It’s Further Along
Plaque, the soft bacterial film that forms on teeth throughout the day, accumulates along and beneath the gum line when it isn’t consistently removed. Left undisturbed long enough, it hardens into calculus that brushing can’t clear. The bacteria within that deposit trigger an inflammatory response in the surrounding gum tissue. That’s where gum disease starts.
In its earliest form, the inflammation is confined to the soft tissue. Bone and connective tissue aren’t involved yet. The signs it produces are subtle: slight redness, some puffiness, bleeding when the gums are brushed or probed. Subtle enough that most patients either don’t notice or notice and assume it will settle.
What separates gum disease from most dental problems is the nature of what it destroys. Decay reaches the nerve and produces pain that eventually becomes impossible to ignore. Gum disease breaks down the bone and connective tissue supporting the tooth gradually, and those structures don’t carry the same nerve supply that signals acute pain. Significant bone loss can occur over months or years without the patient feeling it happen.
The absence of pain is not evidence that the condition is stable or absent. It’s a feature of how the disease progresses, and it’s the main reason patients arrive at a more advanced stage than they needed to.
What the Signs Actually Look Like Before It Becomes Obvious
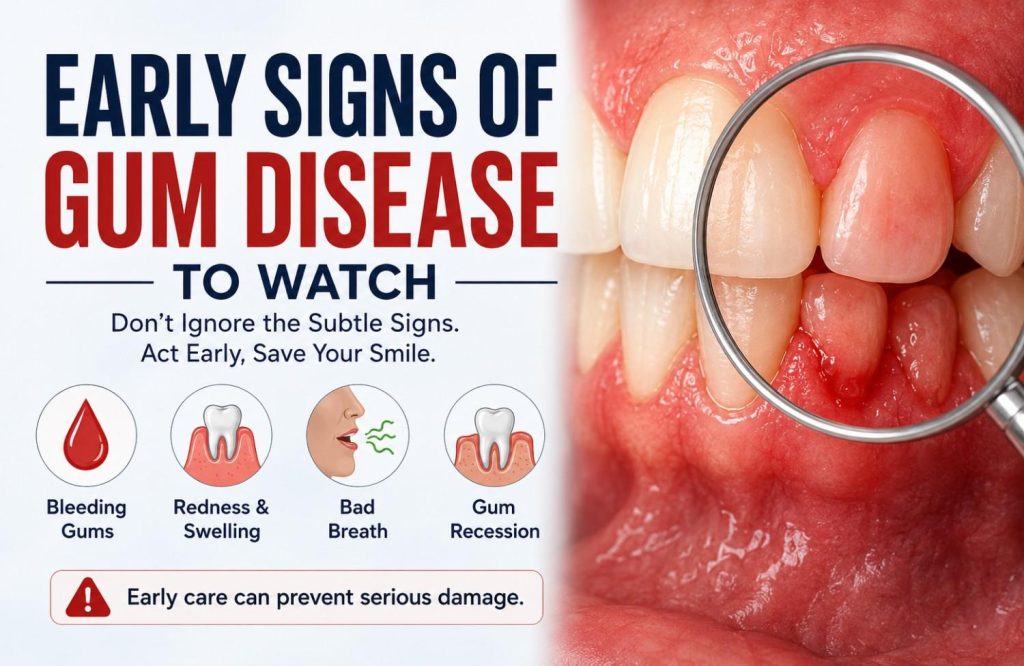
Each of the following signs has a plausible innocent explanation most people apply automatically. That’s exactly why they’re worth examining more carefully.
- Bleeding gums during brushing or flossing. Healthy gums don’t bleed in response to normal cleaning regardless of brushing pressure. When gums bleed consistently, even occasionally, it’s the tissue responding to bacterial inflammation beneath the gum line, not a technique problem. The frequency is what matters: a one-off episode is different from something that happens reliably.
- Redness or a purple tinge along the gum margin. Healthy gum tissue is a firm coral pink and fits tightly against the tooth surface. Tissue that looks redder, darker, or more saturated reflects increased blood flow to chronically inflamed gums.
- Swollen or puffy gum margins. A healthy gum margin has a crisp, tight edge where it meets the tooth. Inflamed tissue loses that tightness, becoming rounded and edematous. The change is subtle enough to miss unless you’re looking for it.
- Tenderness along the gum line. Not sharp pain, a sensitivity to touch or pressure along the margin that wasn’t there before. It indicates active inflammation in the tissue before it has progressed to deeper structures.
- Gum recession. The gum line pulling back from the crown of the tooth, exposing more of the root surface than was previously visible. Recession often happens gradually enough that it goes unnoticed until one tooth looks noticeably longer than its neighbors.
- Persistent bad breath that brushing doesn’t resolve. Bacterial activity within periodontal pockets produces volatile sulphur compounds. Mouthwash reduces the odor temporarily. It doesn’t reach the source.
- A recurring bad taste with no obvious cause. Often connected to the same bacterial activity, particularly when a pocket has become more actively infected.
Bleeding gets attributed to a new toothbrush. Recession gets attributed to age. Bad breath gets attributed to diet. None of these explanations are unreasonable on their own. They become a problem when they’re used to avoid an assessment that would settle the question in a single appointment.

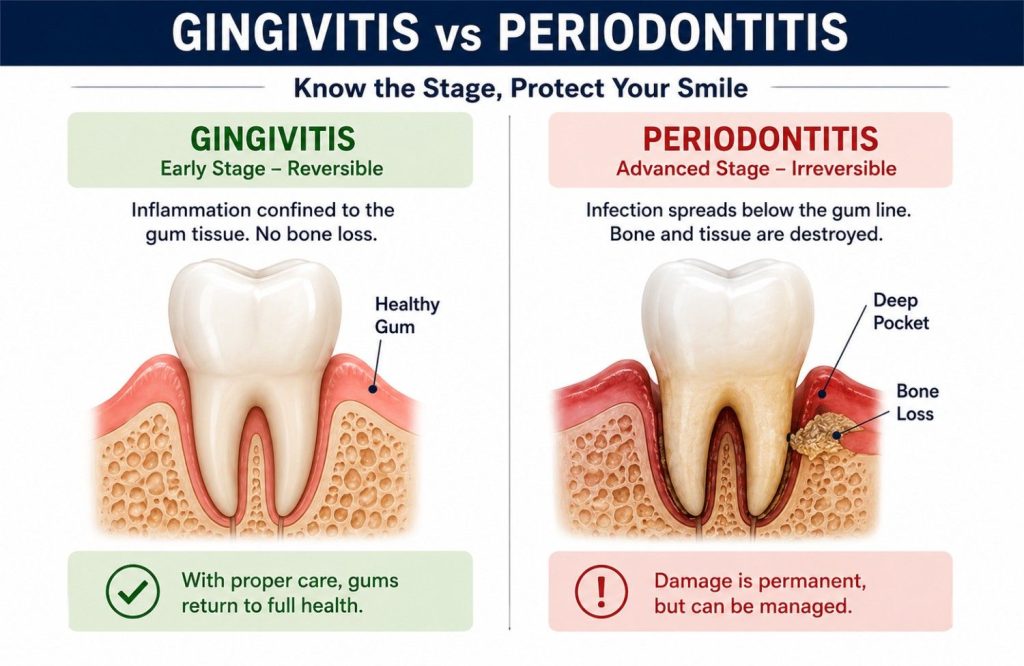
The Difference Between Gingivitis and Periodontitis
The stage gum disease is at determines what treatment looks like and what outcome is realistic. That distinction matters more than most patients realize when they’re first told they have it.
Gingivitis is inflammation confined to the gum tissue. Bone and connective tissue anchoring the tooth aren’t involved yet. At this stage the damage is reversible. Professional cleaning to remove the calculus and plaque driving the inflammation, combined with consistent home care, typically returns the tissue to full health. No bone has been lost. The condition, caught here, is fully resolvable.
Periodontitis is what gingivitis becomes without intervention. The infection spreads below the gum line into bone and connective tissue. Periodontal pockets deepen as tissue is destroyed, creating a sheltered environment where bacteria accumulate and the condition progresses further. Bone lost to periodontitis doesn’t fully regenerate. The disease is managed rather than reversed, and managed well it remains highly stable, but the baseline is permanently lower than it would have been at the gingivitis stage.
The shift between the two doesn’t produce a noticeable signal. No new symptom, no pain, no visible change that marks the transition. It happens below the gum line over a timeline that varies considerably between patients. Immune response, genetics, smoking, systemic health, and oral hygiene habits all influence how quickly or slowly the progression occurs.
The only way to know which side of that line you’re on is a clinical assessment with probing measurements and X-rays.
The difference between gingivitis and periodontitis is the difference between reversible and irreversible. That distinction is what makes the timing of assessment matter.
The Systemic Connection Most Patients Aren’t Told About
Periodontal disease is classified as a dental condition. Its consequences extend well beyond the mouth.
Inflamed gum tissue at the pocket lining is ulcerated, which gives bacteria and bacterial byproducts a direct route into the bloodstream. In a healthy mouth that pathway is largely closed. In a mouth with active periodontitis it’s continuously open.
The cardiovascular link is the most extensively researched. People with periodontitis carry a statistically higher risk of heart disease and stroke. The mechanisms proposed include direct bacterial seeding of arterial tissue and the chronic systemic inflammatory state that periodontal infection sustains contributing to atherosclerosis. The relationship is substantial enough that cardiologists and periodontists increasingly treat the two conditions as connected rather than parallel.
The relationship with diabetes runs in both directions. Poorly controlled blood sugar impairs the immune response to periodontal bacteria, making diabetic patients more susceptible to gum disease and slower to respond to treatment. Active periodontal infection simultaneously makes blood sugar harder to control. Managing gum disease in a diabetic patient produces measurable improvements in glycemic control, which is why the connection matters clinically in both directions rather than just one.
Periodontitis has also been associated with adverse pregnancy outcomes. Periodontal bacteria and inflammatory mediators have been identified in amniotic fluid, and the link between active gum disease and preterm birth or low birth weight is documented well enough to warrant periodontal assessment as part of prenatal care.
For anyone managing diabetes, cardiovascular disease, or a pregnancy, gum disease isn’t a separate concern in a different category. It’s part of the same health picture.
How Untreated Gum Disease Progresses
Untreated gingivitis progresses to periodontitis in patients who are susceptible to it. The timeline varies. The direction, without intervention, doesn’t.
As periodontitis advances, the pockets between the tooth and gum deepen. Deeper pockets shelter more bacteria, create conditions where harder-to-treat anaerobic organisms thrive, and become increasingly difficult to disrupt with normal oral hygiene. Bone loss continues as long as the infection is active. The tooth loses attachment incrementally, without signaling that it’s happening.
Mobility is usually the first sign a patient notices that something has structurally changed. A slight looseness when biting, a tooth that moves when pressed. By the time mobility is detectable, the supporting bone loss is already significant. Chewing patterns shift to compensate, placing additional load on adjacent teeth and accelerating bone loss in surrounding areas.
Gum abscesses develop when infection within a deep pocket becomes acute. Localized swelling, pain, and sometimes discharge; these are often the first symptoms severe enough to bring a patient in who has been ignoring earlier signs. At that point the condition has progressed considerably beyond where it needed to reach before treatment began.
Periodontitis is the leading cause of tooth loss in adults globally, ahead of decay. The progression that leads there starts with the signs covered in this blog and moves through stages that are all more manageable earlier than later.
What Gum Disease Treatment Looks Like at Each Stage
What treatment involves depends almost entirely on the stage the disease is at. For most patients who seek care at the point of noticing the early signs, it’s considerably less involved than they’ve assumed.
At the Gingivitis Stage
A professional scale and polish removes the plaque and calculus deposits that brushing can’t reach, clearing the bacterial trigger driving the inflammation. Combined with improved interdental cleaning at home, this is typically sufficient to reverse gingivitis completely. Gum tissue responds within weeks. Bleeding reduces, color normalizes, puffiness resolves. The condition at this stage doesn’t require anything beyond a cleaning appointment and a change in home care routine.
At the Periodontitis Stage
Scaling and root planing goes further than a standard clean. Carried out under local anesthesia, it removes bacterial deposits from root surfaces within the periodontal pockets, smooths the root to encourage tissue reattachment, and reduces pocket depth to a level that home oral hygiene can maintain. Most patients describe it as more thorough than a regular cleaning rather than painful. Some tenderness in the days following is expected as the tissue responds.
Maintenance is what follows active treatment and what keeps the condition stable long term. Periodontal bacteria repopulate over time; regular maintenance appointments disrupt that cycle before pockets deepen and bone loss resumes. The interval between appointments is determined by how the individual patient’s condition responds.
Surgical intervention is an option for cases where non-surgical instrumentation can’t adequately access deep pockets, or where bone regeneration is a realistic goal. It’s not the default starting point.
A gum disease consultation in Abu Dhabi establishes the stage, maps the pockets, and determines what treatment is actually needed before any assumptions are made about what that involves.
Next Step
Gum disease at the gingivitis stage is fully reversible. At the early periodontitis stage it’s highly manageable. The signs covered in this blog, bleeding that recurs, recession that’s progressing, bad breath that doesn’t respond to brushing, are worth taking seriously at the point they’re noticed rather than at the point they’ve become harder to ignore.
For most patients the harder part isn’t the treatment. It’s closing the gap between noticing something and having it assessed. One appointment establishes what’s actually happening beneath the gum line, which stage the condition is at, and what addressing it involves.
That picture is a considerably less complicated one to sit with than the uncertainty of not knowing. Gum disease treatment in Abu Dhabi starts there.