General dentists and orthodontists both offer teeth straightening. Both can be certified Invisalign providers. Both can place braces. From the outside, the treatments look similar, and the price difference between practitioners isn’t always easy to read in terms of what it actually reflects clinically.
The training difference is specific and it translates to specific clinical advantages in specific situations. It doesn’t make general dental orthodontic practice inadequate. It makes certain cases the domain of a practitioner whose training was built around them. Understanding which cases those are is what the practitioner decision actually requires.
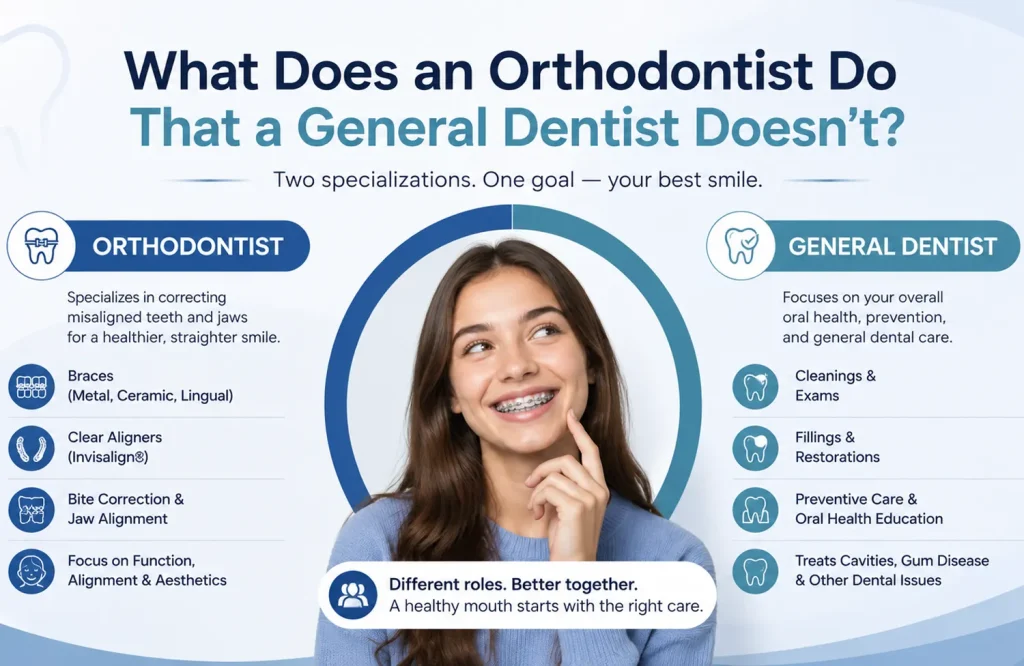
The Training Difference, Specifically
An orthodontist completes a dental degree and then a postgraduate specialty program in orthodontics: two to three years of full-time clinical and academic training that covers territory general dental education doesn’t reach.
Cephalometric analysis is one of the core components. Cephalometric X-rays produce standardized lateral skull images from which skeletal and dental relationships are precisely measured. The angles and distances describe the spatial relationship between the upper and lower jaw, the position of teeth relative to the jaw bones, and the soft tissue profile. A treatment plan that accounts for those relationships, and what the proposed tooth movement will do to them, is built on a diagnostic picture that general dental training doesn’t include at that depth.
Growth modification requires understanding how the developing craniofacial skeleton responds to orthodontic forces during specific windows of development. Certain appliances can redirect jaw growth, but only during the growth period, and only when the timing and the intervention are matched to what the developing face needs. Identifying those windows and using them appropriately is a postgraduate clinical skill. The same finding in a ten-year-old and a twenty-five-year-old has different treatment implications, and knowing what those implications are is what the training builds.
Complex biomechanics cover the management of tooth movement across the full arch in three dimensions: maintaining anchorage while applying force in multiple directions, planning for the changes treatment produces across the jaw, and managing cases where the mechanical demands exceed what a limited range of aligner or bracket use addresses. The clinical exposure concentrated into a specialty program builds that understanding at a level that orthodontic continuing education added to general dental practice doesn’t replicate.
The formal outcome of the postgraduate program is specialist registration, a credential that distinguishes a practitioner who has completed that pathway from one who has completed general dental training with orthodontic courses added.
Where General Dental Orthodontics Works Well
General dentists with additional orthodontic training and accumulated clinical experience can competently manage a defined range of cases. A significant number of patients receive successful orthodontic outcomes from general dental providers, and the cases where that works well share identifiable characteristics.
The malocclusion is dental rather than skeletal: the problem is tooth position, not jaw position. Crowding or spacing is mild to moderate. The periodontium is healthy, with no significant bone loss or gum disease that would complicate tooth movement. The patient is an adult or older adolescent with a fully developed skeletal base, removing the growth modification variable from the clinical picture entirely.
Clear aligner systems like Invisalign have been designed to function within general dental delivery at the mild-to-moderate complexity end of the range. The software-driven treatment planning, where the aligner sequence is generated from digital scans and tooth movements are pre-programmed, reduces some of the clinical variable in straightforward cases. A general dentist treating mild crowding with Invisalign in a patient who fits the profile above is working within a legitimate and appropriate clinical scope. The maintenance and care demands of that treatment are covered in detail in How to Clean Invisalign Aligners Without Damaging Them.
The relevant variable isn’t whether the practitioner is a general dentist or an orthodontist. It’s whether the specific case complexity matches the specific practitioner’s training and experience. A general dentist with a focused orthodontic practice and substantial case volume has a different competency profile from one treating occasional aligner cases within a broader general practice. Case complexity relative to practitioner experience is the frame that produces a more accurate assessment than practitioner type alone.
The Cases Where the Training Difference Actually Matters
The cases where specialist training produces a different clinical outcome aren’t defined by severity alone. They’re defined by what the case introduces: skeletal involvement, periodontal compromise, a growing patient, or an interdisciplinary requirement. Each of those variables changes what the treatment plan needs to account for in ways postgraduate orthodontic training specifically prepares for.
Skeletal discrepancies are the clearest example. A bite problem that originates in jaw position rather than tooth position requires cephalometric analysis to establish what’s happening at the skeletal level and what correction is achievable through tooth movement alone. Some skeletal discrepancies can be partially compensated by repositioning teeth. Others require orthognathic surgery, a combined orthodontic and surgical approach where the orthodontist plans and manages tooth movement around the surgical intervention. Neither the diagnostic nor the treatment planning demands of skeletal cases sit within general dental training.
Severe crowding requiring extractions changes the biomechanical picture significantly. Closing extraction spaces while maintaining facial balance and correct final tooth positions requires precise anchorage management across the full arch. The three-dimensional changes extraction treatment produces, and the planning required to control them, are covered at depth in postgraduate training in a way that continuing education orthodontic courses don’t replicate.
Periodontal involvement changes the treatment parameters. Moving teeth in a patient with existing bone loss requires lighter forces, longer intervals between adjustments, and coordination with periodontal treatment to confirm attachment stability before and during tooth movement. The intersection of orthodontic and periodontal treatment planning is postgraduate curriculum. General dental orthodontic practice typically treats patients with a healthy periodontium and refers cases where significant bone loss is present.
Relapse cases, patients returning after significant movement from their treated position, frequently sit at the moderate-to-complex end of the range regardless of how the original treatment appeared. The bone remodeling that has occurred since original treatment, the direction and extent of relapse, and what the retention failure reflects about the original case all inform what re-treatment requires. The complexity of a relapse case is often greater than the complexity of the original presentation.
Why Timing Matters More Than Most Parents Realize
Most parents ask when orthodontic treatment should start. The more clinically relevant question is when assessment should happen, because the two points on the timeline are different and the gap between them is where the most time-sensitive decisions sit.
The American Association of Orthodontists recommends orthodontic assessment by age seven. Not because treatment starts at seven, but because the first permanent molars and incisors have typically erupted by that age, providing enough of the developing dentition to evaluate the bite relationship and identify discrepancies that will become structural problems if left unaddressed. Identifying them at seven gives time to act within the windows that close at skeletal maturity.
Interceptive orthodontics addresses developing problems before they become structural. A narrow upper arch that hasn’t reached suture closure can be expanded with a palatal expander. The same arch at skeletal maturity requires surgically assisted expansion. A crossbite redirecting jaw growth in a nine-year-old can be corrected with a relatively simple appliance at that stage. Left until skeletal maturity, the asymmetry it has produced in the jaw and face may require orthognathic surgery to address fully. The intervention at the right window is almost always simpler than the intervention after it has closed.
Growth modification uses functional appliances to influence jaw growth direction during the growth period. An adolescent with a retrusive lower jaw who is still growing is a candidate for forward jaw growth modification. The same patient at skeletal maturity is a candidate for orthodontic camouflage or, if the discrepancy is significant, surgery. The jaw can be influenced during growth. After growth, it can only be repositioned surgically or compensated for with tooth movement.
A seven-year-old brought for an orthodontic assessment isn’t being committed to treatment. The assessment establishes whether a developing problem is present, whether early intervention is indicated, and whether monitoring through the growth period is the appropriate response. In many cases it produces a watch-and-wait recommendation with a specific follow-up schedule. What it provides that a general dental check-up doesn’t is the developmental evaluation that identifies the cases where timing is the variable that matters most.
What Happens After the Braces Come Off
Teeth move toward their pre-treatment positions after orthodontic treatment because the periodontal ligament and surrounding bone haven’t permanently remodeled to the new positions. That tendency doesn’t fully resolve. It’s managed through retention.
Fixed retainers, thin wires bonded to the back of the front teeth, hold position passively. Removable retainers worn at night maintain it when the fixed retainer isn’t present or in use. The current clinical consensus for most patients is indefinite retention, not a defined period until the teeth stabilize, but an ongoing commitment to retainer wear because the tendency to relapse persists. Patients informed that their teeth will hold position without retainers after a specific timeframe are receiving guidance that isn’t consistent with the current evidence base.
Retention planning belongs in the treatment plan, not at the end of it. The type of retention, the combination of fixed and removable, and the monitoring schedule that follows all depend on the original malocclusion, the mechanics used to correct it, and the specific relapse risk those mechanics produce. A significant anterior open bite has different retention requirements from mild crowding. Retention designed around the specific case is different from a generic retainer handed out when the active treatment concludes.
The specialist retention planning distinction follows the same logic as the treatment distinction. A clinician who has managed the full diagnostic and biomechanical picture of a case plans retention against a complete understanding of what was produced and what it’s most likely to lose. Case-specific retention planning requires knowing the case at that level of detail. Whether the treatment was delivered by a general dentist or an orthodontist, the retention protocol should reflect the complexity of what preceded it.
The Practitioner Decision Follows From the Case
The practitioner question doesn’t have a universal answer. A general dentist with focused orthodontic experience treating mild crowding in a healthy adult is the right clinical choice for that case. An orthodontist treating a growing patient with a skeletal discrepancy is the right clinical choice for that case. The case determines the appropriate practitioner, not the other way around.
Skeletal involvement, periodontal compromise, growing patients, interdisciplinary requirements, and significant relapse all sit in specialist territory for the reasons this blog has covered. Patients whose situations include any of those variables benefit from specialist assessment as the starting point rather than as a fallback when general dental treatment hasn’t produced the expected result.
For patients who don’t know which category their case falls into, an assessment establishes it. Not every orthodontic assessment ends with a specialist treatment plan. Some confirm the case is straightforward and that general dental delivery is appropriate. Some identify complexity the patient didn’t know was present. What the assessment produces in either case is a specific picture rather than continued uncertainty about who to see.
An orthodontic consultation in Abu Dhabi is where that picture is established, and where the decision about who should deliver the treatment follows from what the case actually requires.