Few dental procedures carry the kind of reputation a root canal does. It’s become shorthand for something deeply unpleasant, referenced in conversations that have nothing to do with dentistry. Most patients have formed an expectation of the appointment long before they’ve been told they need one.
That reputation has a history, and the history is real. Root canal treatment decades ago was a different procedure. Less precise instruments, less reliable anesthesia, longer appointments. The experience people describe, or the experience their parents described to them, came from that era. The clinical reality has moved considerably since then. The cultural memory hasn’t.
What rarely gets addressed clearly is where the pain actually originates. The severe, throbbing ache that brings most patients to the clinic is the infection inside the tooth, not something the procedure creates. The root canal removes the source of that pain. That distinction is where most of the fear falls apart under examination.
Why Root Canals Got That Reputation in the First Place
Root canal treatment decades ago was a genuinely different procedure, and that’s where the reputation starts.
Local anesthetics were less refined. Delivery techniques were less precise. Achieving full, reliable numbness in a tooth with an active infection was a real clinical limitation, not a failure of effort. Patients felt things during procedures that patients today typically don’t, and root canals, which involve working at the level of the nerve, sat near the top of that list.
The instruments were different too. Manual files worked through narrow, curved canals slowly and with significant chair time. Modern rotary instrumentation uses flexible nickel-titanium files driven by a motor, faster, more precise, and considerably less demanding on the patient. Digital imaging now maps the root canal anatomy in three dimensions before anything begins. Curved roots, additional canals, unusual anatomy, all of it known in advance rather than encountered mid-procedure.
The clinical experience has moved. The cultural memory hasn’t. Someone who had a root canal in the 1980s described it to someone who described it to someone else, and those accounts have been reinforced by decades of passing references in conversation, television, and film. The procedure being described in most of those accounts doesn’t exist in the same form. The fear it generated has proven considerably more durable than the techniques that caused it.
The Infection Is the Problem. The Procedure Is the Solution.
Beneath the enamel and dentin sits a soft inner tissue called the pulp, containing the tooth’s nerves and blood supply. In a healthy tooth it goes unnoticed. When bacteria reach it through deep decay, a crack, or trauma, that changes quickly.
Infected pulp becomes inflamed inside a sealed chamber with no outlet for the pressure building within it. That pressure is what produces the severe, often throbbing pain that characterizes a tooth in need of root canal treatment. It doesn’t respond predictably to over-the-counter medication. It doesn’t resolve on its own. It progresses.
As the infection advances beyond the root tip into surrounding bone and tissue, a periapical abscess develops. The pain shifts character, becoming deeper, more constant, and in some cases accompanied by swelling that spreads into the jaw.
A root canal removes the infected pulp, cleans and disinfects the canal system, and seals it. The source of the pain is eliminated. What follows in the days after treatment is soreness in the surrounding tissue as it settles, not comparable in character or intensity to what preceded the procedure.
Most patients fear what they’re already experiencing. The treatment resolves it.
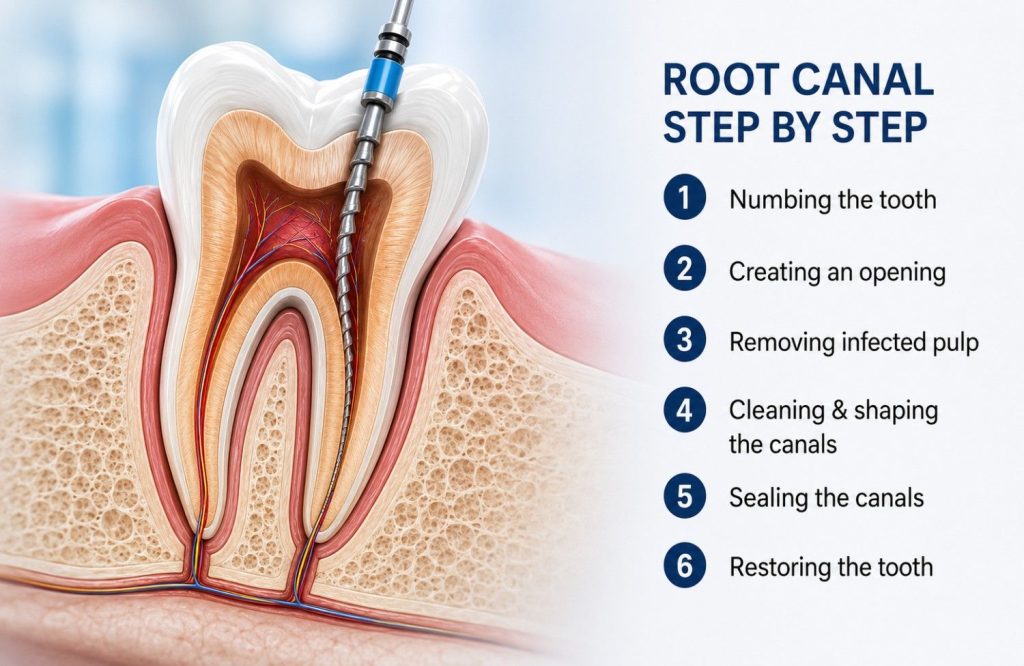
What Happens During the Appointment, Step by Step
Local anesthesia comes first. The tooth and surrounding tissue are fully numb before anything else begins. For most patients the injection is the sharpest sensation of the entire appointment, and it’s the same injection given before a filling.
Once the tooth is numb, a rubber dam is placed around it. A thin sheet of material that isolates the tooth, keeps the field dry, and gives the dentist a clean working environment. It’s routine, and most patients forget it’s there within a few minutes.
A small opening through the crown of the tooth gives access to the pulp chamber. Fine instruments called files remove the infected tissue and shape the canal walls from inside. The canals are irrigated throughout with an antimicrobial solution, clearing bacteria and debris as the work progresses.
When the canals are clean and dry, they’re filled with gutta-percha, a material that seals the space and prevents bacteria from re-entering, and the access point is closed.
A crown typically follows at a separate appointment. Root canal treated teeth lose their internal moisture source and become more brittle over time. On a molar taking the full force of chewing, a crown isn’t optional. On a front tooth, the clinical picture determines whether one is needed.
One to two appointments covers most cases. More complex root anatomy or a severe infection going in can extend that.
During the Procedure, After It, and What’s Normal in Between
With effective local anesthesia, what registers during a root canal is pressure and movement, not pain. The tooth is numb, the surrounding tissue is numb, and the sensation of instruments working inside the canal is present but not acute. Some patients are surprised by how little they feel. Others find the pressure uncomfortable even without pain, particularly during deeper canal work. Both are normal responses to the same procedure.
One situation is worth addressing directly. A tooth with an acute, actively spreading infection can resist local anesthesia more than a healthy tooth does. Inflamed tissue has a lower pH, which affects how the anesthetic binds. An experienced clinician recognizes this, uses supplemental injections or alternative delivery points, and doesn’t proceed until the tooth is adequately numb. That’s not a negotiable step.
In the Hours After
As anesthesia clears, typically two to four hours after the appointment, mild to moderate soreness in the tooth and surrounding tissue is expected. The area has been worked, and the tissue around the root tip responds to that. Ibuprofen or paracetamol manages it in most cases. Some patients need neither.
Soreness tends to peak within the first 24 hours. The tooth may feel sensitive to pressure or touch in that window; avoiding chewing on that side for the remainder of the day is the practical response.
The Days Following
By the second or third day the soreness is usually settling. Some tenderness when biting can persist for up to a week as the tissue around the root tip heals and the periodontal ligament adjusts. That’s within the expected range.
Pain that worsens after day three, swelling that develops or spreads, or fever aren’t part of normal recovery. They’re not common, but they warrant a call to the clinic rather than patience.
What the Alternative to Treatment Actually Looks Like
Avoiding a recommended root canal is a decision many patients make, at least for a while. The fear of the procedure feels more immediate than the problem the procedure would solve. What happens during that delay is worth understanding clearly.
A dental infection doesn’t stabilize. Bacteria within the pulp continue to multiply, the infection progresses through the root tip into surrounding bone, and the pain that brought the patient to the clinic in the first place worsens rather than resolving.
Antibiotics help in a specific and limited way. They reduce the spread of infection systemically and bring acute swelling down. They don’t penetrate the sealed canal system where the source of the infection sits. When the course ends, the infection resumes. The tooth still needs treatment, and the window for straightforward treatment has narrowed.
Prolonged infection causes bone loss around the root. Once the supporting bone is sufficiently compromised, the tooth becomes unrestorable. The option at that point isn’t a root canal. It’s an extraction, followed by decisions about what replaces the tooth, an implant, a bridge, or a gap that affects how the surrounding teeth sit and function over time.
The pain associated with a dental abscess at that stage is categorically different from the soreness that follows a root canal. The procedure most patients fear is considerably more manageable than the situation they’re trying to avoid by postponing it.
Next Step
The reputation root canal treatment carries was earned by a procedure that no longer exists in the same form. What replaced it is faster, more precise, and for the overwhelming majority of patients, far more manageable than what they imagined walking in.
The fear most people bring to the appointment is real. So is the gap between that fear and what the procedure actually involves. For most patients the harder part is making the decision to come in, not the appointment itself.
Anyone sitting with a root canal recommendation and questions that remain unanswered is better served by a direct conversation than continued research. The specifics of a single tooth, its anatomy, the state of the infection, the likely recovery, are particular to that case. A root canal consultation in Abu Dhabi takes less time than most patients expect, and it starts with those questions rather than assuming they’ve already been answered.