Replacing a missing tooth is a decision most people make once and live with for years. The surface comparison between implants and dentures is easy enough: one costs more, one involves surgery, one comes out at night. Most accounts of the two options don’t go much further than that.
The upfront difference is only part of what separates them. What each option does to the jaw over time, how each performs under the daily demands of eating and speaking, what each actually costs across ten or twenty years rather than at the point of treatment, these are the criteria that change how the decision looks.
Neither option is universally better. Which one is right depends on clinical candidacy, long-term goals, and a financial picture that goes beyond the first invoice. That’s the comparison this blog covers.
Two Different Approaches to the Same Problem
A dental implant is a titanium post placed surgically into the jawbone. Over the months following placement, the bone grows around and fuses with the post, a process called osseointegration. An abutment and crown are then attached on top. The finished result is fixed, non-removable, and anchored in the jaw the same way a natural tooth root is. It takes biting pressure directly. It doesn’t shift, require adhesive, or need to be removed. This is part of why implants are a long-term solution for many patients.
Dentures are removable prosthetics that rest on the gum tissue surface. A full denture replaces all teeth on an arch, held in place by suction against the gum and palate. A partial denture replaces some teeth and uses clasps on remaining natural teeth for additional retention. Neither type connects to the bone beneath. They sit above it, supported by tissue that changes shape over time. For a closer look at the types and benefits of dentures, see our full guide.
The distinction between embedded in bone and resting on tissue is what produces the differences in bone health, stability, and long-term function that the rest of this comparison covers.
|
Dental Implants |
Dentures |
|
|
Placement |
Surgically embedded in jawbone |
Rests on gum tissue surface |
|
Removability |
Fixed, non-removable |
Removable |
|
Bone integration |
Fuses with jawbone over time |
No integration with bone |
|
Support structure |
Jawbone |
Gum tissue, suction, or clasps |
|
Function |
Comparable to natural tooth |
Prosthetic appliance |
The Bone Health Question Neither Option Can Ignore
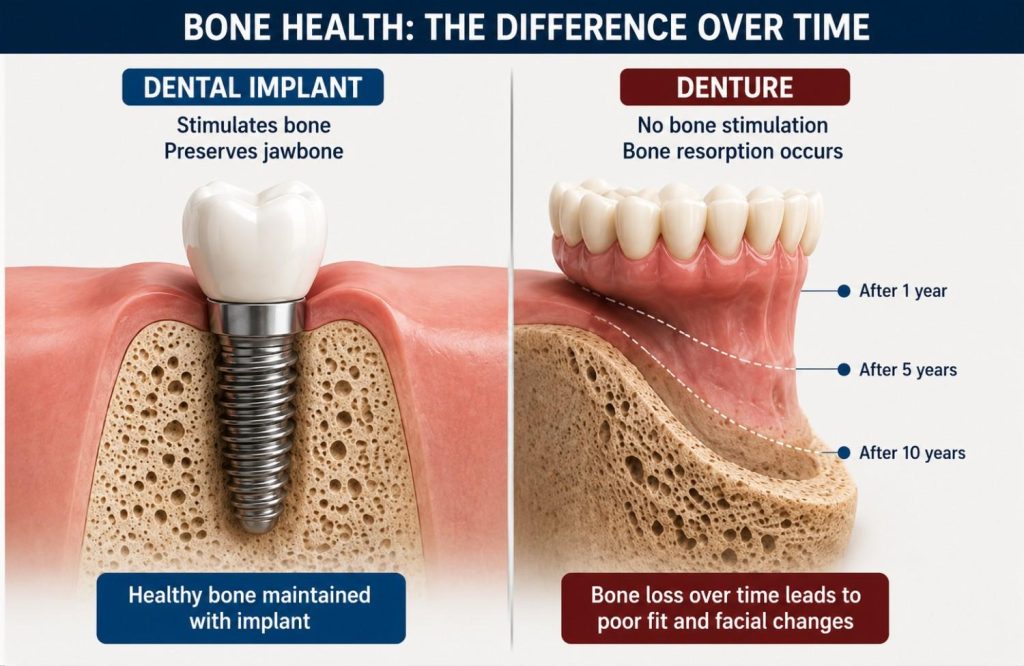
The jawbone maintains its density through stimulation. In a natural tooth, that stimulation comes from the root transmitting biting forces into the surrounding bone with every chew. When a tooth is lost, the stimulation stops. The bone in that area begins to resorb, losing volume progressively. It’s a slow process and largely invisible in its early stages, until it starts affecting adjacent teeth, facial structure, or the fit of whatever is sitting on top of it.
Dentures don’t interrupt that process. They rest on the gum surface and distribute pressure across the ridge, but that isn’t the signal the bone was receiving from a root. Resorption continues beneath a denture regardless of fit. As the underlying bone changes shape, the denture that fit well at delivery begins to loosen. Relining buys time. It doesn’t address what’s driving the change. Patients who have worn full dentures for a decade or more often present with significantly altered jaw profiles: the lower face shortens, the ridge flattens, and retention becomes progressively harder to achieve as less bone remains to support the prosthetic.
An implant post embedded in the jaw changes that picture directly. Bone grows around the titanium and the implant transmits occlusal force into the surrounding structure the way a root does. Resorption in that area is halted or substantially reduced. The jaw maintains its volume around the implant site, which matters for facial structure, for adjacent teeth, and for the longevity of the restoration itself.
Patients who have delayed the implant decision for years sometimes find at consultation that bone loss has progressed far enough to require grafting before placement is viable. Grafting works, but it adds time and cost to the process that earlier intervention would have avoided.
Bone loss beneath a denture is gradual and largely invisible until fit changes or the jaw profile begins to alter. By the time relining is needed, meaningful resorption has already occurred.
Eating, Speaking, and Living With Each Option
Dental Implants
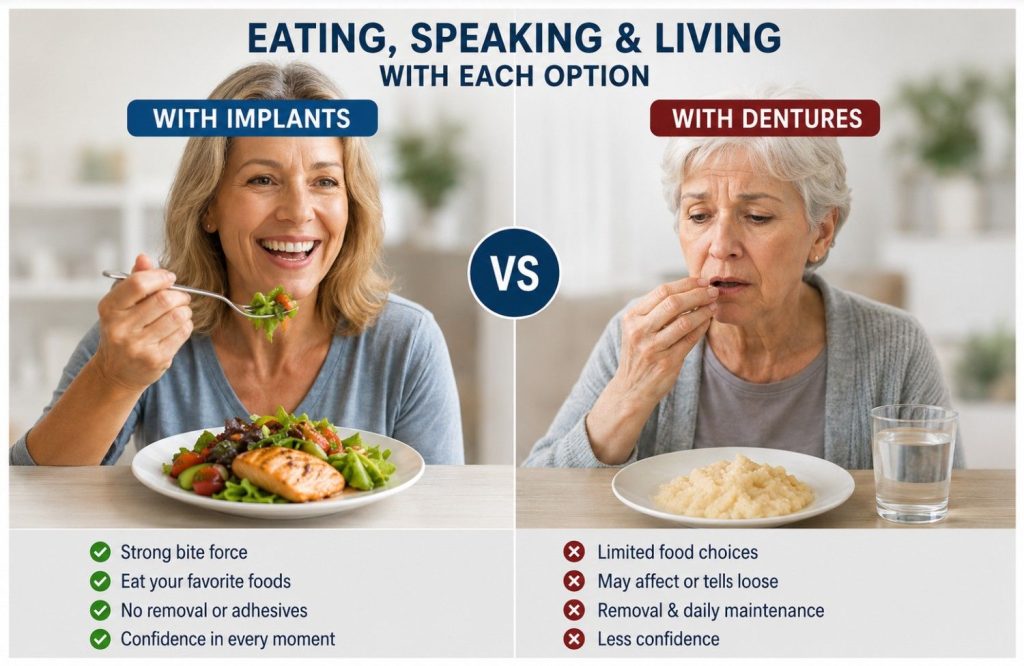
Once integrated, implants function close enough to natural teeth that most patients stop accounting for them within a few months. Bite force returns to something near normal. Foods avoided with dentures, hard vegetables, crusty bread, anything requiring sustained pressure on a specific point, become accessible again. There’s no removal routine, no soaking overnight, no adhesive applied before eating. Oral hygiene is brushing and flossing around the crown the same way as a natural tooth.
The process to get there takes months from surgical placement to final restoration. Once the crown is seated and the implant integrated, no further adaptation is needed.
Dentures
The adjustment period for a new denture is longer than most patients are prepared for. Speech changes initially as the tongue and lips relearn their positions around a different oral environment. Eating requires relearning bite patterns, distributing pressure evenly, and avoiding foods that can dislodge or damage the prosthetic.
Full lower dentures are the most difficult to stabilize. The lower jaw offers less surface area than the upper palate, and tongue movement during eating and speaking works against retention. Adhesives reduce movement but don’t address the underlying fit problem, particularly as the jaw changes shape beneath the denture over time.
Many denture wearers describe a background awareness of stability that doesn’t fully resolve. A formal meal, a conversation that involves laughing, situations where unexpected movement would be noticeable. Whether that awareness fades depends on the individual and how well the denture fits. For patients who never fully adapt, implant-supported options, covered in the next section, change the experience considerably.
Candidacy Is What the Comparison Ultimately Comes Down To
Preference and cost shape the implant versus denture decision. Candidacy often shapes it more.
Bone density and volume is the primary physical requirement. The implant post needs sufficient bone to fuse with. Patients who have had missing teeth for several years may have experienced enough resorption to require bone grafting before implants are viable. Grafting is well established and effective, but it adds a preparatory stage that affects both the timeline and the overall cost.
Gum health needs to be addressed before placement. Active periodontal disease creates conditions where implants are significantly more likely to fail. Gum disease is treated first and the tissue stabilized before implant planning begins.
Systemic health influences outcomes in specific ways. Uncontrolled diabetes impairs healing and affects how bone integrates with the implant. Bisphosphonates, used for osteoporosis, affect bone metabolism in ways that need discussion before treatment planning. Neither is an automatic disqualifier, but both require honest assessment.
Smoking raises implant failure rates meaningfully. Most clinicians counsel against smoking through the healing period and ideally before placement. Patients who smoke aren’t excluded, but the risk profile is different and needs to be factored into the decision.
Age has a floor but not a ceiling. Implants require a fully developed jaw, typically from the late teens onward. There is no upper age limit where general health supports the procedure. Patients in their seventies and eighties receive implants successfully when the clinical picture warrants it.
Patients who don’t currently qualify aren’t necessarily excluded permanently. Bone grafting, periodontal treatment, and better management of systemic conditions can bring someone into candidacy who wasn’t there at the initial consultation. That pathway is worth discussing rather than assuming the door is closed.
The Upfront Price Is Only Part of What Each Option Costs
Implants cost more upfront. That’s the figure most patients focus on, and for many it’s where the comparison ends. The longer view looks different.
The higher initial cost of an implant reflects what the procedure involves: surgical placement, the post, the abutment, the crown, and bone grafting where required beforehand. Once integrated, the post typically remains in place for decades. The crown can be replaced if it wears without touching the implant beneath. Beyond that, maintenance is regular check-ups and normal oral hygiene. There are no scheduled replacement costs built into the treatment structure.
Dentures carry a lower entry cost that recurs. Relining is needed within a few years as the jaw changes shape beneath the prosthetic. Replacement follows, typically every five to ten years depending on wear and how significantly the underlying bone has shifted. Each cycle carries laboratory and clinical costs. The cumulative figure across fifteen or twenty years narrows the gap with implants considerably, and the gap narrows further when bone loss eventually complicates the fit enough to require a new impression and a remade prosthetic.
The costs that don’t appear in either figure are worth acknowledging. Dietary restriction, daily adhesive use, relining appointments, the background awareness of stability that many denture wearers carry. None of those show up in a price comparison. All of them are part of what the option costs across time.
Insurance coverage for implants and dentures in the UAE varies significantly by plan and provider. Confirming what applies before the consultation gives a clearer picture of the actual out-of-pocket comparison.
Next Step
For patients who qualify, implants address the long-term consequences of tooth loss more completely than dentures. Bone health, daily function, and the maintenance picture across ten or twenty years all sit on the same side of the ledger for a candidate whose health and financial situation support the treatment.
For patients who don’t qualify, or for whom the upfront cost is a determining factor, dentures and implant-supported options are legitimate solutions rather than compromises. The stability and bone health gap between conventional dentures and implants narrows considerably with implant-supported systems, at a cost that sits meaningfully below full individual replacement.
What changes at a consultation is specificity. Bone density, jaw anatomy, medical history, the number and position of missing teeth; these details determine which options are viable and what the realistic cost and timeline look like for a particular patient rather than a general case. A dental implant consultation in Abu Dhabi takes the comparison from general to specific, which is where the decision actually becomes answerable.